


le mans rencontre bi Surgery of deafness is preceded by a hearing check-up and an audiometry.
Borzya Tympanoplastie, ossiculoplasty, otosclerosis, cholesteatoma, implantable prosthesis, bone conduction implants, invisible hearing implant (Envoy-Esteem), cochlear implants, otoneurosurgery.
Tympanoplasty includes all restoration techniques of the tympanic membrane and hearing attributable to chronic ear infections.
Most commonly, a retro-auricular route (incision behind the ear – invisible after a few weeks) is practiced; a layer of connective tissue that covers the temporalis muscle (fascia temparalis) is used for the reconstruction of the eardrum.
In case of destruction of an element of the chain of ossicles, the replacement is provided by one of the usable ossicles after it has been reshaped or by a prosthesis made of biocompatible materials.
Bone lesions (osteitis) and skin inclusions (cholesteatoma) in the ear are carefully removed.
A silastic sheet can be placed under the graft to prevent it from sticking.
Small absorbable sponges are placed in the ear canal.
The procedure takes on average an hour and a half; it can be performed under neurolep-analgesia, in ambulatory.
In terms of tympanoplasty, the anatomical results (restoration of the eardrum) are excellent (97%); you can swim or shower without fear of ear flow.
The functional results (improved hearing) are excellent in 70% to 75% of cases depending on the stage and the state in which the ear is at the time of the surgery.
Ossiculoplasty is the repair of the ossicular chain of the middle ear whose role is to pass sound vibrations picked up by the eardrum to the inner ear fluids which, in turn lead to vibrations of the basilar membrane of the cochlea stimulating sensory cells.
Ossicular chain is composed of three bones: the macleus, the incus and the stapes. The destruction of one or more bones during chronic otitis interrupts sound transmission with a hearing loss of up to 60 dB.
The chain reconstruction uses different techniques sometimes by transposing the patient’s own bones or replacing them with prosthetic materials, plastic, ceramic or titanium.
This is a hereditary disease causing progressive deafness commonly due to a fixation of the stapes footplate(usually mobile) in the oval window.
The intervention lasts half an hour and is performed under general or local anesthesia. During the surgery, the eardrum is first retracted through the ear canal in order to reveal the stapes (aka the stirrup).
A 0.6mm-diameter-hole is made in the footplate with a micro-diamond burr or a laser. The immobilized stapes is then replaced by a mobile Teflon piston, attached to the long process of the incus.
After the operation dizziness may occur. The procedure requires a hospitalization for 24 to 48 hours. A week of convalescence might be necessary to get used to the noises and the sound of the world that awaits you. It is essential to protect yourself against loud noises.
The results are excellent (98% to 99% depending on the stage at which the lesion is taken care of). The intervention slows down or even stabilized the progression of the otosclerosis but the ear remains more sensitive to trauma in general, whether acoustic or pressure (IOP).
In the final stage of certain otosclerosis, hearing aids can be fitted after the intervention.
The tinnitus is much improved by the intervention unlike certain whistles that may remain after the intervention although they’ve been alleviated.
Cholesteatoma is a benign tumor due to the skin penetration in the ear cavities which acquires the power to destroy the bone and a tendency for superinfections.
The tumor is entirely eradicated in order to prevent a recurrence. A checkup is usually required a year later.
The natural evolution of the cholesteatoma tends toward various complications such as suppuration, labyrinthine fistula with vertigo, meningitis, facial paralysis…
The same surgical techniques as for tympanoplasty are used.
(BAHA, Medel-vibrant soundbridge, Otologics, Envoy)
Conventional hearing aids have made remarkable progress but can sometimes be inadequate or inappropriate depending on the type of pathology.
The implantable prostheses have developed in two directions: the bone-anchored hearing aids (BAHA) and middle ear prostheses semi-implantable and today fully implantable.
Our experience began over 15 years ago from our multidisciplinary consultation that encompassed bone-anchored prostheses in the rehabilitation of congenital malformations of the ear and cochlear implants indicated in total deafness. The combination of surgical, audiological, radiological, psychological, and speech therapy skills at the Clinique Roosevelt allows to deal with all types of hearing loss (children and adults) and to optimize the functional results.
In 1998, the first semi-implantable prostheses of Symphonix ® (Siemens) type were introduced, followed by the Otologics ® prostheses, indicated in sensorineural hearing loss in order to overcome certain disadvantages of conventional intra-or ear-tipped prostheses (duct obstruction, feedback, skin tolerance, acoustic distortions, poor rehabilitation of trebles; difficulty of understanding in noise …).
In practice, we commonly use three types of semi-implantable prostheses for the rehabilitation of moderate to severe hearing loss:
– Bone anchored hearing aid B.A.H.A,
– Vibrant Soundbridge® (Med-el),
– And the Otologics® hearing aid.
As for fully implantable prostheses, two are available:
– Envoy
– and Otologics®.
Each system has specific indications beyond those of conventional hearing aid because it is now possible to cope with “ski-slope” hearing losses (significant loss of high frequencies) and have a solution for total deafness in one ear.
The purpose of any hearing aid is to vibrate the fluids of the inner ear to stimulate the ciliated cells remaining. The vibration energy can be provided by air or bone conduction, the further the vibrating system from the “otic capsule”, the greater the energy required. This consideration widely broadens the scope of indications for hearing aids to diseases and hearing losses that were until now unsolved and in many cases improves the results compared to conventional prostheses.
This is a direct bone conduction system from a retro-mastoid-transcutaneous implant made of osseo-integrated titanium.
The results are excellent from a good assessment of cochlear reserve in the conductive or mixed hearing loss (with a bone conduction loss below 45 dB) related to a congenital malformation, chronic otitis with mastoid cavity, recurrent otorrhea; inoperable ankylosis of the ossicular chain (single ear, inoperable, elderly), in cases of eczema of the duct and in case of unilateral deafness.
A free-field hearing test through a vibrator can show the patient the desired result and assist decision-making.
Introduced in France in 1987, it now represents 40% of bone conduction prostheses.
Progress on glasses or conventional vibrators (headband) is important: no absorption of high frequencies by the soft tissues beyond 2500 Hz, a direct and effective conduction without any distortion, without fluctuation due to changes in position; without pain or irritation due to the pressure of a vibrator against the skin as the anchoring ensures the stability of the device and patient safety.
The titanium screws of 3 or 4 mm, is placed under local anesthesia in one surgery time. A Biogaze bandage surrounding the screw, held by a plastic flange is repeated a week later and removed the following week.
The first adjustment is made after six weeks; enough time for a perfect osseo-integration.
For long, the otologist found himself helpless when dealing with unilateral cophosis (total deafness on one side) however it now represents a new indication to restore a pseudostereophony.
The sound is collected by the microphone on the deaf side and transmitted through bone conduction to the healthy opposite ear to eliminate the masking effect of the head (about 30 dB) and restore a sense of binaural hearing particularly interesting for the recent cophoses highly resented by patients (sudden deafness, after a translabyrinthine surgery approach to treat acoustic neuromas …)
BONEBRIDGE system – a new system of stimulation through bone conduction
This implant system is bone conduction hearing system totally innovative suitable for people with hearing loss, mixed hearing loss or unilateral deafness. This system transmits sounds to the inner ear by bone conduction, in order to “bypass” the problems at the outer ear or middle ear. It includes an external component and an internal component.
Bonebridge system is a semi-implantable hearing system, the implant being placed entirely under the skin. Signals are transmitted to the implant via an external audio processor, comfortably worn under the hair.
Bonebridge system, respecting the integrity of the skin, may be an alternative to transcutaneous BAHA according to the anatomy of the mastoid and surgical sequelae.
The Esteem®-Hearing Implant™ is 100% implantable and therefore invisible.
This implant uses the ear drum as a natural microphone for a better understanding of speech. There is no physical microphone so no interference, no feedback, and no occlusion effect because there is nothing in the ear canal.
The device is implanted under the skin behind the ear. Two leads extend into the middle ear from the device. Sound waves travel into the ear canal and set the ear drum (tympanic membrane) into motion causing the bones of the middle ear to vibrate. The device senses these movements and delivers a customized dose of energy to the cochlea which transmits the signals to the brain.
Most of the hearing impaired, resist the use of conventional hearing aids as there is a negative social stigma attached with them. Interestingly, with the Esteem®- hearing implant, the patient is completely unaware of its presence in their body. More importantly, beyond the aesthetic aspect, this new technology allows patients to hear naturally and restores their life to normal living.
Another advantage is that the product is maintenance free for 5 to 9 years. The average lifespan is 6 ½ years (for a 16h/day and 7/7 use)
Like every normal and healthy ear, this device leverages the body’s natural anatomy. Due to the basic laws of physics and human physiology, attempts with artificial methods to improve hearing, such as hearing aids, do not possess this capability. This is the only treatment that takes into account hearing loss and aesthetic aspect. The result is that patients describe a clarity and fidelity of sound that is near normal.
Background Noise: This is the one of the biggest complaints for people wearing hearing aids. Taking part in a conversation at a restaurant, with a group of friends, at a business meeting are usually the most difficult situations for hearing aid wearers. Yet, these are situations they want most to be a part of, the social, active and interactive part of life.
Patients using the Esteem hearing implant report easier listening, better understanding and more enjoyment in life, regardless of their background environment.
Testimonies gathered by Esteem Company
“I can hear sounds that I had not perceived for years”
“There may be many people at the table, I can, even if someone calls me from afar and asks me a question, locate it, I can hear his question and I can answer him.»
“I listened and understood in black and white and now with the Esteem ® implant it is in color.”
“The surgery is virtually painless.”
Two other implantable prostheses apply vibration directly on the mobile ossicular chain. They are suitable for losses up to 80 dB at high frequencies.
These implants have two main advantages compared to conventional prostheses:
The first is not to obstruct the external ear canal
And the second is the possibility of treble restoration up to 8000 Hz with low acoustic distortion and an excellent sound discrimination of ambient noise.
Patients who want maximum comfort without external elements can opt for fully implantable hearing aids.
In cases of hearing loss with preservation of bass frequencies, such as the ski-slope hearing loss (mainly high frequencies loss), only an implantable hearing aid is indicated with a clear sound quality. Low frequencies are perceived in a natural way, and high frequencies rehabilitated with little distortion.
Indeed, a conventional hearing aid that clogs the duct would cut the lows to re-amplify them with a lower quality and would not amplify frequencies above 3000 Hz because of resonance problems in the external ear canal.
Open fit digital hearing aids overcome this drawback when the hearing loss is not too important with a restoration up to 4500 Hz.
In case of high frequency loss above 60 dB, conventional hearing aid wearers often complain of being uncomfortable in noisy environment (restaurant) or with multi speakers (cocktail party) because they do not perceive the high frequencies that would allow them to emerge from the noise.
Moreover, the high level of acoustic energy delivered by conventional hearing aids causes echoing, saturation, feedback with an ear fatigue.
A final point is the easy fit with low maintenance, simple adjustments, and listening comfort.
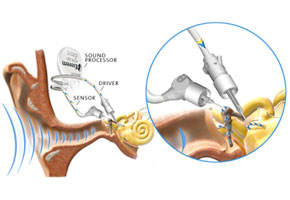
The Middle ear implants (Vibrant Soundbridge ® Med-el and Otologics ®) are semi-implantable prostheses for the rehabilitation of moderate to severe sensorineural hearing loss. It is based on the direct transmission of sound to the ossicular chain. This innovative principle greatly improves sound quality and thus intelligibility.
The outer part contains the microphone, the electronic chip similar to a digital prosthesis and the magnet which allows a comfortable fit in front of the receiver implanted behind the pinna. The transmission to the receiver is done by magnetic induction through the skin. These systems are usually offered to adults over 18 years dissatisfied with conventional hearing aid or as a first-line treatment for an optimal rehabilitation.
Middle ear implants have the advantage of releasing the external auditory canal and avoiding the problems caused by occlusions as well as improving the physical comfort. It also removes the resonance phenomena when chewing for instance.
Low frequencies pass through the natural ways without over-amplification. Direct transmission to the chain is more effective with a wider bandwidth of up to 8000 Hz, while the frequency response of a conventional external hearing aid microphone over 3 to 4 500 Hz is very limited.
There are fewer distortions and no feedback problems given the distance between the microphone and the vibrator. Patients describe sounds and their own voices as more natural, ambient noises are better tolerated and above all they feel a great improvement of discrimination in noise.
The procedure is performed under general anesthesia. The first adjustment occurs after 6 to 8 weeks. It is fundamental to note that there is no need for habituation. The listening comfort is immediate. The Vibrant Soundbridge Med-El hearing aid is particularly suited to high-frequency hearing impairments with conservation of low frequencies.
The Otologics hearing aid which is more powerful is designed for higher low-frequency losses and more severe hearing loss. The latter became fully implantable with a microphone and an internal rechargeable battery, so no external element. A new hearing aid called “ENVOY” is available and fully implantable with different characteristics.
The cochlear implant is a device suitable for profound or total deafness.
The sound information is transmitted directly to the auditory nerve fibers in the cochlea in the form of electrical stimulations that are then analyzed and interpreted by the auditory cortical areas of the brain.
The equipment includes an implanted part (receptor and electrodes) and an external part in the form of a BTE (microphone, processor and battery) that transmits information to the internal coil by magnetic induction.
Several implants are available: Neurelec (MXM), Cochlear (NUCLEUS), MEDEL BIONICS (CLARION)…. They have proven their efficiency and safety for more than 25 years.
Preliminary tests should be made to evaluate the patient’s degree of auditory perception.
Our specialized team assesses the prognosis by measuring the patient’s ability to analyze the information transmitted. Indeed, the organization of the auditory pathways and the brain plasticity determine the outcome in terms of discrimination. Tests developed at the Clinique Roosevelt allow individual prognosis before surgery.
A 48 hour-hospitalization is sufficient for a 1h30min-operation under general anesthesia.The postoperative course is simple, without pain or vertigo, the patient whether an adult or a child (early intervention by the age of 8 months) can leave the following morning. The bandage and stitches are removed after one week.
The first adjustment is made between 15 days and one month after surgery. The processor is set individually according to the wearer’s hearing needs. It is programmed using a special computer by our acoustic engineer.
The electrodes inserted into the cochlea to stimulate the auditory nerve are adjusted to respond to a particular intensity or height depending on the patient’s auditory responses. It is essential that the auditory perception is pleasant, comfortable and informative.
However, as the auditory perception changes over time, the speech processor can be adjusted again as often as necessary. For children, a true hearing education performed by Speech Language Pathologists (SLPs) is necessary for best results.

(Neuroma, dizziness, facial paralysis)
Otoneurosurgery includes surgery of the sensorineural structures of the ear and of the cerebellopontine angle, or acoustic-facial bundle surgery that is:
– The surgery of vertigo (vestibular neurectomy);
– The surgery of facial paralysis (decompression, graft);
– The surgery of tumors of the auditory nerve in the internal auditory canal and in the cerebellopontine angle (acoustic neuroma)
– Auditory brainstem implants
Otoneuro-surgeries are performed by an otoacoustic neurosurgical team (neurosurgeon + otologist) with cranial nerves monitoring systems and radiological neuro-navigation (MRI, SCANNER).